Dal seguente documento dell'Istituto Superiore di Sanità utilizzato da molte ASL per rassicurare i genitori sull'alluminio negli alimenti e nei vaccini si dice
In [ ] le citazioni ufficiali del documento
http://www.epicentro.iss.it/temi/vaccinazioni/pdf/Le_domande_difficili_2015.pdf pag. 18-19
[ I sali di alluminio invece non sono eliminabili dai vaccini che attualmente li contengono, perché giocano un ruolo fondamentale nella risposta immunitaria (senza di essi l’efficacia di alcuni vaccini sarebbe fortemente ridotta); il contenuto di alluminio nei vaccini è dell’ordine di alcuni mg (variabile, a seconda del prodotto, da 0.25 a 2.5 mg). ]
Purtroppo non è così
fonti

[ L’Organizzazione Mondiale della Sanità (World Health Organization 1997b) afferma che nella popolazione generale non esiste alcun rischio sanitario in relazione all’assunzione di alluminio con i farmaci e con l’alimentazione (ogni giorno ingeriamo con il cibo dai 5 ai 20 mg di alluminio, che è contenuto soprattutto nei vegetali; parte della quantità di alluminio ingerita va in circolo e viene eliminata per via renale); la tossicità da alluminio è riscontrabile solo nei lavoratori professionalmente esposti e in alcuni pazienti affetti da insufficienza renale cronica i quali, a causa della loro malattia, non riescono ad eliminare l’alluminio per mezzo dei reni. ]
In questo studio
"The aluminium content of infant formulas remains too high"
fonte
http://bmcpediatr.biomedcentral.com/articles/10.1186/1471-2431-13-162
gli autori hanno analizzato il contenuto di vari latti in polvere e liquidi commercializzati in plastica, tetrapak etc. ed hanno trovato in molti prodotti valori di alluminio oltre i valori massimi consentiti.
"The concentration of aluminium in each of the 30 infant formulas is at least twice that which is recommended in the European Union for drinking water (50 μg/L) and in 14 of the milks it exceeds the maximum admissible level for drinking water of 200 μg/L
fonte http://dwi.defra.gov.uk/stakeholders/legislation/wqregs2007cons.pdf
. While these recommended values for aluminium in drinking water were, historically at least, not set with human health as a criterion, they are used today in general practice to ascertain whether or not potable waters are fit for human consumption
fonte http://dwi.defra.gov.uk/stakeholders/legislation/wqregs2007cons.pdf
We consider that the aluminium content of all infant formulas investigated herein is too high and especially so considering that these products constitute either all or a substantial proportion of an infant’s diet in the first months of their lives. Based upon the criteria for drinking water they are not fit for human consumption and they contravene article 5 of the Food Safety Act which states that ‘infant formulas should not contain anything which might endanger the health of infants and young children’".
fonte
http://www.legislation.gov.uk/uksi/2007/3521/pdfs/uksiem_20073521_en.pdf
Per cui gli autori concludono che prendendo come riferimento le normative per la potabilità dell'acqua molti prodotti non potrebbero essere utilizzati per consumo umano.
Ne deriva che essendo l'alimentazione nei primi mesi di vita dei neonati a base di questi prodotti una grande concentrazione di alluminio potrebbe recare danni alla salute, considerando anche il calendario vaccinale.]
Il lattante ingerisce quotidianamente alluminio: esso si trova nel latte materno, ad una concentrazione media di 40 microgrammi per litro, mentre il latte artificiale presenta una
concentrazione più elevata, in media 225 microgrammi per litro e il latte di soia una concentrazione variabile tra 460 e 930 microgrammi per litro (Keith 2002). Solo una piccola parte dell’alluminio ingerito passa nel sangue, ossia meno dell’1% (per la precisione, lo 0.78%)
Se si seguono le raccomandazioni del calendario vaccinale, un bambino italiano riceve nel primo
anno di vita:
3 dosi di esavalente: ogni dose contiene 0.82 mg di alluminio, per un totale di 2.46 mg
3 dosi del vaccino contro lo pneumococco: ogni dose contiene 0.125 mg di alluminio, per un totale di
0.375 mg.
Totale per tre dosi dei due vaccini: 2.8 mg, quindi meno di 3 millesimi di grammo.
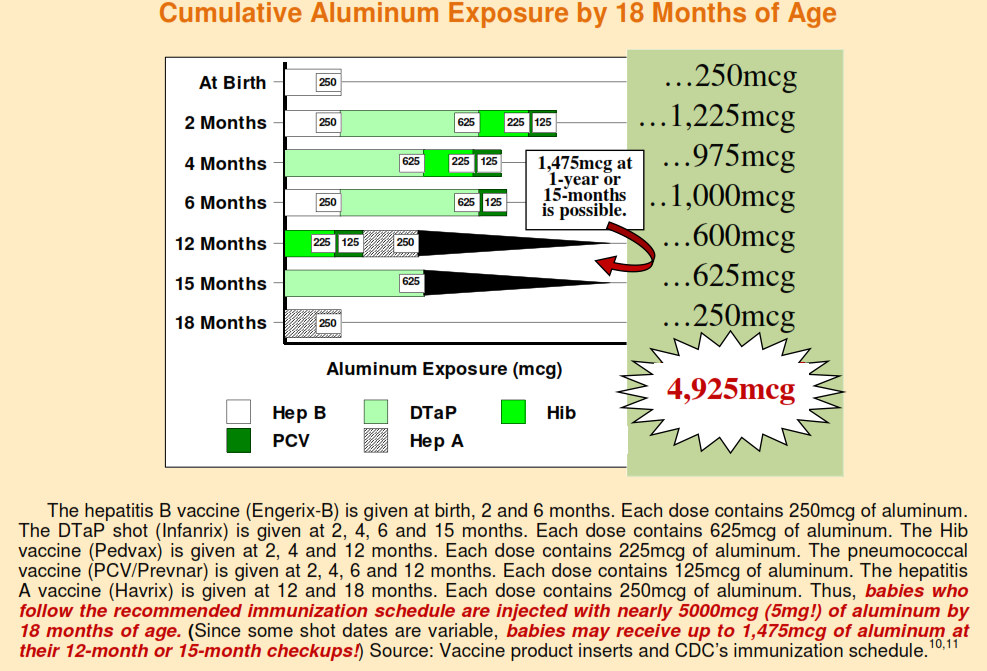
[ Purtroppo le cose non stanno esattamente così
fonti
10. CDC. “Recommended childhood immunization schedule for persons aged 0-6 years, United States, 2009.”
11. Data on aluminum content is taken directly from the manufacturers’ product inserts.
Nella seguente pubblicazione
Aluminum toxicity in infants and children (RE9607),” Pediatrics (March 1996);97(3):413-416.
fonte: http://pediatrics.aappublications.org/content/pediatrics/97/3/413.full.pdf
gli autori sostengono che
"Aluminum is now being implicated as interfering with a variety of cellular and metabolic processes in the nervous system and in other tissues" ]
L’alluminio iniettato nel muscolo con i vaccini non entra immediatamente nel sangue, come erroneamente riportato da alcuni.
In realtà una parte (sino al 51%) è assorbita gradualmente nel sangue durante i primi 28 giorni, mentre la restante parte entra un po’ per volta in circolo e viene
smaltita nelle settimane successive (Mitkus 2011).
ipofunzionalità epatica e renale consentirà all'alluminio di raggiungere il cervello anche perchè la BBB è ipofunzionale? Abbiamo sopra visto che grandi quantità di alluminio sono introdotti dai neonati attraverso i vaccini
( quasi 5 grammi nei primi 18 mesi ) e nella enorme contaminazione del latte prodotto per l'età pediatrica ]
Ciò significa che l’organismo del lattante ha un lungo periodo di tempo per smaltire gradualmente l’alluminio iniettato con i vaccini e quindi la quantità iniettata, di per sé molto
piccola, non raggiunge mai concentrazioni considerate tossiche.
Il carico corporeo di alluminio derivante dai vaccini e dalla dieta per tutto il primo anno di un bambino di vita è significativamente inferiore al livello di sicurezza stabilito dall'Agency for Toxic Substances and Disease Registry, l’agenzia federale americana che si occupa del rischio chimico (Mitkus 2011).
Tra i vaccini pediatrici correntemente utilizzati, solo l’antipolio, l’anti-Haemophilus b e l'anti-morbillo-parotite-rosolia non contengono sali di alluminio.
[ Nel seguente studio
J Pediatr. 2007 Aug;151(2):167-72. Epub 2007 Jun 22.
Primary immunization of premature infants with gestational age <35 weeks: cardiorespiratory complications and C-reactive protein responses associated with administration of single and multiple separate vaccines simultaneously.
gli autori sostengono ( Pourcyrous study )
A plausible explanation for variation in the magnitude of CRP responses to immunization may be attributed to viral versus bacterial antigenic stimulation, minor variability in the quantity of antigens in different vaccine lots, the multiple antigenic component of a vaccine, the presence and the quantity of aluminum adjuvant, genetic polymorphism or to decrease immunologic responses in some preterm infants. [24]
Overall, 16 percent of infants had potentially lethal vaccine-associated cardio-respiratory events with episodes of apnea (cessation of breathing) and/or bradycardia (abnormal slowing of the pulse). Intraventricular (brain) hemorrhages occurred in 17 percent of those receiving single vaccines and in 24 percent of those receiving multiple vaccines.
considerando che il carico di alluminio è massivo nel lattante per le ragioni sopradescritta, è improbabile che il lattante possa espellerlo in toto considerando una naturale immaturità della metilazione, epatica e renale, per cui vi è un accumulo nei tessuti fra i quali quello nervoso. L'alluminio è neurotossico e altera pesantemente il metabolismo cellulare ]
La dr.ssa Dr Suzanne Humphries in queste sue slide sintetizza la tossicità dell'alluminio nei vaccini
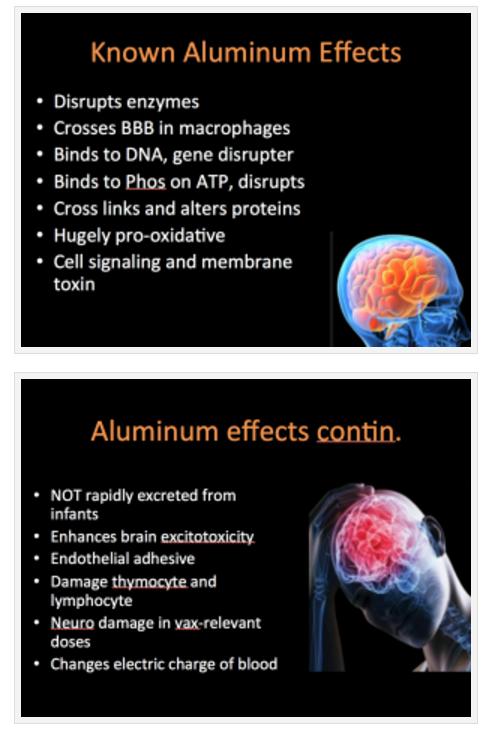
http://www.vaccinationcouncil.org/2015/02/20/video-of-dr-suzanne-humphries-aluminum-is-toxic-to-all-life-forms-the-case-against-aluminum-in-vaccines/
per le alterazioni neurobiologiche ed approfondimenti si vada qui
http://emedicine.medscape.com/article/165315-overview
a voi i commenti del caso
 Salvatore Morelli
Salvatore Morelli








Inserted
Skipped
None
Removed